
Even Daniel Alfredsson can't skate off a numb leg
Because medical school doesn't occupy enough of my time, I've been blogging over at Puck, That Hurts! about the medical aspects of hockey. Last Tuesday's announcement that Daniel Alfredsson would be undergoing back surgery can only mean one thing: It's time for Silver Seven and Puck, That Hurts! to collide.

Time heals all wounds. Actually, it's time, physical therapy, medication, possibly surgery, and not pushing yourself for no reason.
In a show of truly spectacular self-defeatism, talented hockey players will often push themselves to come back before their body is ready. How often do we hear about someone "Playing through it"? And why are some injuries somehow more acceptable to play through than others? Nobody would expect a player to suit up after an eye injury or a giant laceration (Clint Malarchuk, anyone?), but this year we saw player after player limping through the playoffs on injuries that should have had them out for the duration. Was Dany Heatley really contributing more by playing with a broken hand and a high ankle sprain than he would have by packing it in for the season? Was that one point in the Western Conference finals worth the pain? If you asked him he'd probably say yes. How about Steven Stamkos – he hurt his shoulder in the Pittsburgh series, and played through to the Eastern Conference Finals where he tallied seven points. So absent of my sneaking suspicion that Stamkos is basically infinitely better than Heatley (sorry, Sharks fans), for him it probably was worth it.
 |
Daniel Alfredsson was the perfect example this year (and last) of playing with injuries that should have put him in the press box. Ottawa Senators fans scratched their heads and wondered what was wrong as their captain's point production dropped off towards the end of the 2009-10 season. After the Sens were eliminated in the first round of the playoffs (as usual) by the Pens, Alfie admitted he'd been playing with a sports hernia since February (which isn't really a hernia, but groin pain caused by any number of different injuries in the… ahem… area). He still finished the season with 71 points, more or less on par with his usual production.
This year Alfie only played 54 games, and finished with 31 points – the fewest games and points he's put up since he started with the Sens in 1995-96. The problem this time was a back injury that he tried to fight through, and to which he finally conceded defeat in early February. He admitted he'd been having weakness in his right leg, and Tuesday Ottawa GM Bryan Murray made the following statement:
"Daniel will have surgery on Friday. He's done a lot of rehab. He felt to continue his career at the level he wants to, it's the right thing to do. It's just to relieve a little pressure on the nerve that has taken away some of the strength in his leg and affected his skating and overall game, obviously… It was a decision that he, during the latter part of the year and the off-season now, was hoping that he wouldn't have to have. I guess the fact the nerve is touching and being affected … in particular on the left side of his body … that he felt it was the right thing after much thought."
 |
The Injury
Although the interviews disagree on which leg was affected, the common thread is that Alfredsson has a lower back injury that's causing one of his legs to be weak, tingly, and "heavy". Murray said today that there was pressure on a nerve that needed to be relieved. The best way to understand why an injury in the back is affecting the leg is to learn a little something about the spine and dermatomes.
Whatatomes?
The nerves that make up the spinal cord exit the vertebrae through little canals called intervertebral foramina and proceed on to whatever part of the body they're responsible for. Those parts are very specific, and beautifully demonstrated by this fellow:
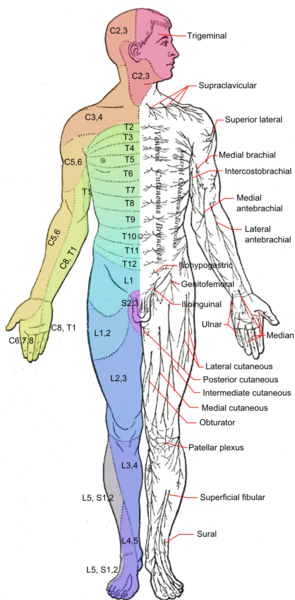
Each zone on the dermatome map represents the area that the specific listed nerve innervates. So if you hurt L4 or L5, the top of your foot will suffer for it.
The Spine Story
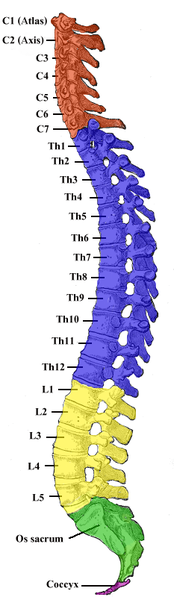 |
You have 24 vertebrae, plus 9 more that are fused to form the sacrum and coccyx (which make up the back wall of your pelvis). The vertebrae are lettered and numbered according to where they are. From the top, you've got:
- Cervical (neck) C1-C7
- Thoracic (midback) T1-T12
- Lumbar (lower back) L1-L5
- Sacral (S1-S5 – fused) and coccygeal (also fused, don't have a fancy letter, but have the distinction of being the oft-whacked tailbone).
The spinal nerves are named for the associated vertebra. Those among you who are clever (or smartasses) have probably already noticed that although you have seven cervical vertebrae, there are eight cervical spinal nerves. Feel free to impress girls at (nerdy) parties with the following bit of spine trivia: The spinal nerves exit the vertebral column above the associated vertebral bone until nerve C8 – the first one to exit below the bone (specifically vetebra C7) – cleverly paving the way for an extra nerve.
Bored yet?
The vertebrae are cushioned by discs, which are tough cartilage rings around a jelly-like center. It's a great design – they're shock absorbers, allow for movement, and hold things together. Unfortunately, they can also get badly out of place and cause awful symptoms.
When good discs go bad…
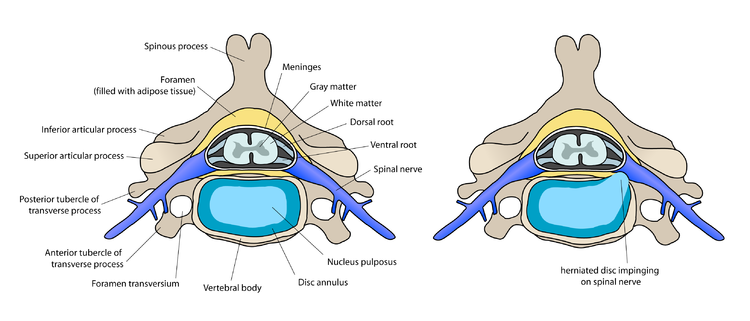
Injury or aging can cause discs to go to new and exciting places (that you'd rather they didn't visit). You can have a disc bulge – where the outer cartilage ring sticks out (usually posteriorly) from between the vertebrae and can put pressure on spinal nerves (or the spine itself). A bulge can become a herniation, where the outer cartilage ring loses integrity completely and the jelly-like inside protrudes. These injuries are best seen on MRI, like so:
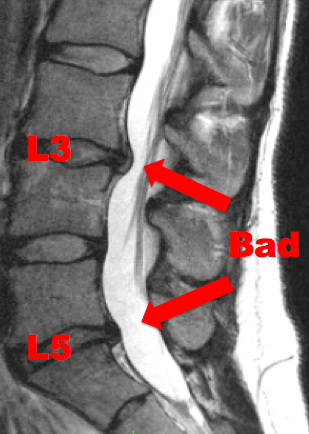 |
These are disc bulges at L3 and L5 – very common places for this type of injury. This particular injury was the result of lifting a fat drunk kid out of a deep ditch in the rain after he drove mommy's Lexus off the road. But I'm totally over it. Obviously. I actually got lucky – I've been able to stay functional with exercise, responsible NSAID use, and being smart about lifting – let the fire department do it! Kidding. Sort of. Not really.
If you look at the information available, it should be clear to you at this point that Alfredsson most likely has a disc bulge or herniation that's pressing on one of his lumbar nerve roots. He tried rehabbing the injury for a long time, and in fact there's good data to show that non-surgical treatments are usually very effective for this sort of injury. Pain control, steroids to relieve inflammation and physical therapy can bring relief in the majority of patients. The exception is patients who have symptoms exceeding six weeks despite appropriate treatments, specifically those with neurologic deficits – Weakness, sensory deficit (numbness), and tingling. This is Alfredsson's picture. Obviously he tried far longer than six weeks to avoid surgery, which was smart. He also made loud noises after the all-star break about wanting to come back and play out the end of a dismal season, which was dumb. There was no point, and there would have been a risk of worsening the injury.
(FYI... According to the World Health Organization, spinal manipulation (chiropractics) in the setting of a disc herniation is contraindicated.)
The Surgical Fix
If Alfie does indeed have a herniation that's pressing on a spinal nerve root, the likelihood is that he'll be having a discectomy of some sort. The operation is exactly what it sounds like: Part of the disc is removed. First a laminectomy is performed, where a tiny portion of the lamina (part of the vertebra) is removed to allow access to the disc and nerves. The actual disc surgery can be done as an open procedure (cut the back open, remove part of the disc), percutaneously (through a small incision in the skin – less effective than open), or as microdiscectomy (where the surgeon operates using a special microscope allowing for more precise cuts and thus less damage to surrounding tissues). A retractor holds the nerve roots out of the way while a device called a rongeur (one of my favourite medical words - it's French for gnawer) removes the offending disc tissue. This should relieve the pressure on the nerve, allowing a return of strength and relief of pain. The material that's removed in surgery will eventually fill itself in with new disc material.
 |
A study out of Dartmouth cleverly called SPORT (Spine Patient Outcomes Research Trial) showed that patients with lumbar herniations showed significantly more improvement in pain and functionality with discectomy than patients who used non-surgical interventions. Remember: These are the people with symptoms that persisted longer than six weeks with neurological problems and failure of non-surgical treatment.
After the surgery patients are encouraged to get up and walk as soon as possible, and physical therapy is started two weeks post-op. It consists of stretching, strength training, and all the usual torture PTs put patients through (I love PTs, but they're giant bullies – just ask one).
What we learned…
Alfredsson took from February until June to decide that he needed back surgery. Although I admire his attempts to keep from being operated on, the research shows that if he was still having symptoms after six weeks he would have been better off just having the discectomy. Did his hesitation stem in large part from his clear (and often-stated) desire to come back and play at the end of the season? Probably. With any luck, he'll be looking at about a six-week recovery, which puts him back in action at the end of July. This should have him good to go for training camp on what some think could be his last season with the Sens.
Get well soon, Alfie.
- Jo
Puck, That Hurts! is your home for discussion of NHL injuries during play, hockey health policies and equipment issues. You can also find me on twitter - @JoNana.


